All published articles of this journal are available on ScienceDirect.

Relationship Between Lung Cancer and Mycobacterium Avium Complex Isolated Using Bronchoscopy
Authors Info & Affiliations
Abstract
Introduction:
The incidence of Mycobacterium avium complex (MAC)-positive respiratory specimen cultures and MAC lung disease (MACLD) is increasing worldwide. This retrospective study aimed to assess the association between MAC culture-positive bronchoscopy specimens and lung cancer.
Materials and Methods:
The medical records of 1382 untreated lung cancer patients between 2003 and 2011 were collected using our hospital database. Of them, records for 1258 that had undergone bronchoscopy together with sampling for mycobacterial culture were reviewed. Patient characteristics were compared between those with MAC-positive/other nontuberculous mycobacteria (NTM)-negative bronchial washings and those with MAC-negative/other NTM-negative bronchial washings. Patients with MAC-positive lung cancer were cross-sectionally divided into MACLD and non-MACLD groups, and their features were assessed. Follow-up data for patients with lung cancer but without MACLD were reviewed for subsequent development of MACLD.
Results:
Of the 1258 patients with lung cancer, 25 (2.0%) had MAC-positive/other NTM-negative bronchial washings. The proportion of women (52% vs 30%; P = 0.0274) and patient age (72 years vs 69 years; P = 0.0380) were significantly higher in the MAC-positive/other NTM-negative lung cancer group (n = 25) than in the MAC-negative/other NTM-negative lung cancer group (n = 1223). There were 10 patients with lung cancer and MACLD and 15 without MACLD; significant differences in patient characteristics were not found between the two groups, and none of the 15 patients without MACLD subsequently developed MACLD.
Conclusion:
MAC culture-positive bronchial washing is positively associated with lung cancer. Female sex and advanced age, but not lung cancer characteristics, were found to be associated with MAC infection in patients with lung cancer.
INTRODUCTION
Nontuberculous mycobacteria (NTM)-associated lung disease (NTMLD) is a major cause of morbidity and mortality, with a steadily increasing worldwide incidence [1, 2]. The mycobacteria species isolated in NTMLD vary geographically; however, Mycobacterium avium complex (MAC) is the most frequently isolated species in many countries [2-4]. In Japan, MAC lung disease (MACLD) accounts for approximately 80% of all NTMLDs [4, 5]. Various factors are associated with NTMLD, including environmental factors and host factors, such as thoracic skeletal abnormalities, rheumatoid arthritis, previous pulmonary tuberculosis, bronchiectasis, chronic obstructive pulmonary disease, and lung cancer [2, 6]. Lung cancer is a comorbidity in 4-7% of patients with respiratory NTM (primarily MAC) isolates [7, 8]. However, MACLD in patients with lung cancer has rarely been investigated [9]. Recently, Lande et al.[10]. reported that 25% (62/249) of patients with lung cancer have respiratory cultures positive for MAC. It is important to gain insight into the relationship between MAC-positive cultures and lung cancer. However, patients with pulmonary diseases, including lung cancer, often do not have sputum-associated symptoms; thus, sputum examination for acid-fast bacilli is often not conducted for lung cancer cases. Indeed, in a recent report, sputum culture for mycobacteria was only performed in 15% (249/1632) of patients with lung cancer [10]. Therefore, current estimates of the sputum culture MAC-positivity rate in lung cancer is based on incomplete or inaccurate data.
In Japan, fiberoptic bronchoscopy is usually performed to obtain a definitive diagnosis of MACLD as well as pulmonary tuberculosis [11-13] in sputum-negative patients. Furthermore, because Japan is a middle-ranked country for pulmonary tuberculosis prevalence [14], bronchial washings collected during bronchoscopy are routinely cultured for mycobacteria to diagnose pulmonary diseases, including lung cancer. Although cross-sectional frequency using MAC-positive cultures in bronchial washings is not intended to reflect the overall frequency of MAC positivity in lung cancer, comorbid lung cancer is simultaneously diagnosed in the majority of patients with MAC-positive cultures [9, 10]. In most lung cancer patients, bronchoscopy is performed at diagnosis; thus, simultaneous diagnosis of the two diseases may be obtained by bronchoscopy. Therefore, in considering the MAC-positive rate in lung cancer, assessment of MAC-positive bronchoscopy cultures is important.
The aim of the present retrospective study was to assess the relationship between MAC-positive bronchoscopy samples and lung cancer.
METHODS
Patients and Clinical Setting
We retrospectively reviewed a total of 1,382 consecutive cases of lung cancer admitted to the National Hospital Organization, Tokyo National Hospital between January 2003 and December 2011. Of these patients, 1,258 met the inclusion criteria: 1) initial bronchoscopy was performed to obtain a diagnosis of lung cancer with sampling for mycobacterial culture; 2) chest computed tomography (CT) to increase diagnostic accuracy was undertaken before bronchoscopy; and 3) bacterial, radiographic, pathological, and other clinical data were available from the medical records. Thus, mycobacterial data from the initial bronchoscopy with sampling for mycobacterial culture were analyzed. The case flow diagram is shown in Fig. (1).
There were 106 patients who did not undergo bronchoscopy because of a poor performance status and a definite diagnosis using other samples such as malignant pleural effusions. CT images from before bronchoscopy and other various data were obtained from our hospital databases (lung cancer database, bacteriological database, and other medical records).
Sample Collection and Diagnosis
Fiberoptic bronchoscopy was carried out by experienced physicians via the transoral or transnasal route under local anesthesia and sedation according to the standard procedures: 1) complete inspection of the tracheobronchial trees, including subsegmental bronchi; 2) sampling with bronchial brushings of the bronchial segments at which the target lesion was located on CT; 3) sampling of bronchial and/or lung biopsy from the same segments; and 4) collection of bronchial washings at the orifices of the same segment and related lobe.
Fresh samples of bronchial washings were submitted to the bacteriology and pathology divisions of our facility. For bacteriology, part of each sample was prepared as smears on glass slides and was examined for acid-fast bacilli. The remaining sample was subjected to rapid genetic diagnosis of mycobacteria using a polymerase chain reaction (PCR; Roche, Basel, Switzerland) assay until May 2009 and using a transcription-reverse transcription concerted reaction (TRC; Tosoh, Tokyo, Japan) assay starting in June 2009. For samples that were positive for Mycobacterium tuberculosis on PCR and/or TRC, no further genetic tests were performed. For samples that were negative for M. tuberculosis on PCR and/or TRC, PCR for M. avium and M. intracellulare or TRC for MAC was performed. All samples with or without positive PCR and/or TRC results were cultured for mycobacteria using mycobacteria growth indicator tubes (BACTEC MGIT 960: Becton, Dickinson and Company, Franklin Lakes, NJ, USA). Finally, mycobacterial species were identified using DNA-DNA hybridization (Kyokutoseiyaku, Tokyo, Japan). DNA-DNA hybridization of NTM-positive samples was entrusted to the physicians.
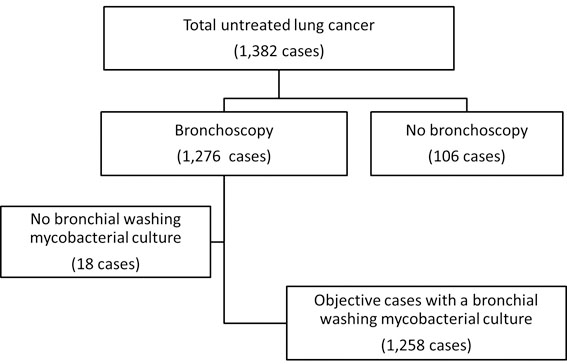
Flow diagram of patients with lung cancer receiving bronchoscopy between 2003 and 2011.
At our hospital, bronchoscope contamination and associated infection are prevented by sterilization with an endoscope reprocessor (OER-2; Olympus, Tokyo, Japan) containing 0.3% ethaneperoxoic acid (Acecide; Saraya, Osaka, Japan), which is a very effective mycobactericidal agent for disinfecting bronchoscopes [15].
Data Compilation and Analysis
The patients were divided into MAC-positive/other NTM-negative group, MAC-negative/other NTM-positive group, and MAC-negative/other NTM-negative group. Based on the NTMLD criteria (two positive sputum cultures or one bronchoscopy or lung biopsy culture with clinical and radiographic features) of the American Thoracic Society and Infectious Diseases Society of America [16], the MAC-positive group and other NTM-positive group were further cross-sectionally divided into MACLD/NTMLD (with characteristic radiographic features) and non-MACLD/ NTMLD (without characteristic radiographic features) groups.
We investigated the lung cancer status at the time of the confirmation of the culture results from bronchial washings in MAC-positive/other NTM-negative patients. The lung cancer status included surgical data after the bronchoscopy. Subsequently, the features of MAC-positive/other NTM-negative lung cancer patients and MAC-negative/other NTM-negative lung cancer patients were compared and analyzed using our hospital database. Next, in the MAC-positive/other NTM-negative lung cancer patients, we compared the lung cancer status between the MACLD lung cancer patients and the non-MACLD lung cancer patients. In addition to the cross sectional analyses, follow-up data for lung cancer patients with MAC-positive non-MACLD were analyzed for subsequent development of MACLD.
Statistical Analysis
All statistical analyses were conducted using R Statistical Software version 3.0.2. Intergroup differences were evaluated using univariate analysis by means of the independent samples t-test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables, as appropriate. Multivariate analyses were included in the logistic regression analysis and performed using the backward elimination method. Differences were considered statistically significant at P < 0.05.
Our institutional review board approved the study (December 24, 2013; approval number 130053), and patient informed consent was considered unnecessary. This study was conducted in accordance with the Declaration of Helsinki.
RESULTS
MAC Positivity in Lung Cancer Patients
Among the 1,258 patients evaluated, 25 (2.0%) had MAC-positive/other NTM-negative cultures, 10 (0.8%) had MAC-negative/other NTM-positive cultures, and the remaining 1223 had both negative cultures for MAC and other NTM. Among the 10 MAC-negative/other NTM-positive cases, there were two cases with M. kansasii-positive, two with M. gordonae-positive, one with M. szulgai-positive, and in the remaining five cases, NTM-species were not identified. Only two among 10 M. kansasii-positive cases met the NTMLD criteria.
The characteristics of these MAC-positive/other NTM-negative patients are summarized in Table 1.
Characteristics of the 25 MAC-positive/other NTM-negative patients with lung cancer.
| Case Number | ||
|---|---|---|
| Sex | ||
| Female/Male | 13/12 | |
| Median age (IQR), years | 72 (67–78) | |
| Smoking | ||
| Yes/No | 14/11 | |
| Lung cancer | ||
| Type | Peripheral/Hilar | 22/3 |
| Location | UL/ML/LL | 15/1/9 |
| Histology | AD/SQ/Others | 18/4/3 |
| Stage | III-IV/I-II | 15/10 |
The predominant clinicopathological features of the 25 lung cancer patients with MAC-positive cultures were female sex (n = 13), smoking history (n = 14) and advanced age (median age, 72 years; IQR, 67 years–78 years). Lung cancers were predominantly of the peripheral type (n = 22), were located in the upper lobe (n = 15), were adenocarcinomas based on histology (n = 18), and were at clinical stage III–IV (n = 15).
Univariate analysis of the clinical features of MAC-positive/other NTM-negative lung cancer and MAC-negative/other NTM-negative lung cancer.
| Background | MAC- Positive/other NTM-Negative Lung Cancer (n = 25) |
MAC- Negative/other NTM-Negative Lung Cancer (n = 1,223) |
Odds Ratio |
95% Confidence Interva | P-Value | |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Female | 13 | 371 | 1 | 0.0274 | ||
| Male | 12 | 852 | 0.402 | 0.182–0.889 | ||
| Median age (IQR), years | 72 (67–78) | 69 (63–75) | 1.053 | 1.003–1.105 | 0.0380 | |
| Smoking | ||||||
| No | 11 | 309 | 1 | 0.0623 | ||
| Yes | 14 | 888 | 0.443 | 0.199–0.986 | ||
| Unknowna | 0 | 26 | ||||
| Lung cancer | ||||||
| Type Hilar | 3 | 307 | 1 | 0.1637 | ||
| Peripheral | 22 | 916 | 2.458 | 0.731–8.268 | ||
| Location UL | 15 | 622 | 1 | 0.5194 | ||
| LL | 9 | 482 | 0.774 | 0.336–1.784 | ||
| Others | 1 | 119 | 0.348 | 0.046–2.663 | ||
| Histology AD | 18 | 731 | 1 | 0.4651 | ||
| SQ | 4 | 274 | 0.593 | 0.199–1.767 | ||
| Others | 3 | 218 | 0.559 | 0.163–1.915 | ||
| Stage I-II | 10 | 560 | 1 | 0.6862 | ||
| III-IV | 15 | 663 | 1.267 | 0.565–2.842 | ||
We compared the 25 patients with lung cancer who were MAC-positive/other NTM negative with the 1223 MAC-negative/other NTM-negative patients. In the univariate analysis, the number of women was significantly higher in the MAC-positive lung cancer group than in the MAC-negative lung cancer group (13/25 vs. 371/1223; P = 0.0274). MAC-positive/other NTM-negative patients were also significantly older than MAC-negative/other NTM-negative patients (72 years vs. 69 years; P = 0.0380). In contrast, positive smoking history, lung cancer type, location, histologic type, and clinical stage were not significantly different between the MAC-positive and MAC-negative lung cancer groups (Table 2).
In the multivariate logistic regression analysis, female sex (odds ratio [OR], 0.388; 95% confidence interval [CI], 0.175-0.860; P = 0.0198) and older age (OR, 1.054; 95% CI, 1.005-1.105; P = 0.0309) were associated with MAC-positive cultures (Table 3).
Multivariate analysis (backward elimination variable selection) for MAC-positive/other NTM-negative lung cancer and MAC-negative/other NTM-negative lung cancer.
| Odds Ratio | 95% Confidence Interval | P-Value | |
|---|---|---|---|
| Sex | 0.388 | 0.175-0.860 | 0.0198 |
| Age | 1.054 | 1.005-1.105 | 0.0309 |
The 25 patients with MAC-positive lung cancer were divided into two groups: those with MACLD (n = 10) and those without MACLD (n = 15). There were no significant clinicopathological differences between these two groups.
Status of the 10 patients with lung cancer and comorbid MACLD.
| Case Number | |
|---|---|
| Type of MACLD | |
| Nodular/bronchiectatic | 8 |
| Fibrocavitary | 1 |
| Others | 1 |
| Spread of MACLD | |
| Multiple lobes | 9 |
| Single lobe | 1 |
| Anatomical relationship between MACLD and lung cancer | |
| Same lobe | 7 |
| Another lobe | 3 |
| Diagnosis of MACLD and lung cancer | |
| Concurrent | 8 |
| Lung cancer sequential to MACLD | 2 |
| Sputum culture for MAC | |
| Positive | 5 |
| Negative | 5 |
Details on comorbid MACLD in the 10 lung cancer patients are presented in Table 4.
Eight of the 10 MACLD patients exhibited nodular/bronchiectatic types on CT, and MACLD had spread into multiple lobes in nine cases. As the nodular/bronchiectatic type of MACLD had spread into other lobes from the origin in the middle lobe and lingula, the anatomical relationship between MACLD and lung cancer involved the same lobe in seven patients; however, there were no patients where the two diseases coexisted within the same lesion. Of the 10 patients with MACLD, two had the disease several years before being diagnosed with lung cancer, while for the remaining eight patients lung cancer and MACLD were detected concurrently. Two patients with lung cancer sequential to MACLD and three of the eight concurrent cases also had MAC culture-positive sputum just after bronchoscopy. There were no cases with disseminated MAC diseases.
Follow-up of Non-MACLD Patients with Lung Cancer
We evaluated the medical data of the 15 patients with lung cancer but not MACLD to determine whether MAC positivity in bronchial washings was a MACLD precursor. All 15 patients with lung cancer received their initial and subsequent lung cancer treatments at our hospital. The median follow-up time was 50 months (range, 37 months-60 months) for 6 patients with stage I-II lung cancer who underwent lobectomy and 12 months (range, 3 months-59 months) for 9 patients with stage III-IV lung cancer who underwent chemotherapy and/or radiotherapy. Among the 6 lobectomy cases, there was only one case with comorbid, non-caseous, epithelioid granulomas surrounding the lung cancer with no acid-fast bacilli in the resected materials; however, the remaining 5 cases had no characteristic MACLD pathologic findings. During the follow-up period, sputum cultures were examined for mycobacteria at least once in all 15 patients. All of the patients had MAC-negative cultures and no radiographic findings compatible with MACLD; accordingly, they did not undergo a second bronchoscopy. Thus, none of the patients had comorbid MACLD.
DISCUSSION
This retrospective study has revealed for the first time a 2.0% rate of MAC-positive bronchial specimen cultures in patients with lung cancer with comorbid lung cancer and MACLD observed in 0.8% of patients with untreated lung cancer who had received bronchoscopy. These results are comparable with our previous report [9].
MAC-positive patients with lung cancer in the present study were more likely to be women, older, and smokers. Further, MAC-positive lung cancers were predominantly peripheral adenocarcinomas, clinical stage III–IV, and located in an upper lobe. However, only female sex and old age were significantly associated with MAC-positive lung cancer when compared with MAC-negative lung cancer patients. Female sex and advanced age, well-known risk factors for MACLD [3, 7, 8, 17], were also associated with MAC infection in patients with lung cancer rather than with lung cancer status.
The clinicopathological features of MAC-positive patients in the present study were generally consistent with those reported by Lande et al. [10], with the exception of the predominance of adenocarcinoma. In our previous study of patients with comorbid lung cancer and NTMLD from 1997 to 2002, smoking history, male sex, squamous cell carcinoma, and fibrocavitary disease on radiographs were predominant clinicopathological features [9]. The predominance of adenocarcinoma in MAC-positive lung cancer patients in our current study might be related to the recent increase in MACLD in Japan. Indeed, the incidence of nodular/bronchiectatic disease in non-smoking females has markedly increased as compared with the previous predominance of fibrocavitary disease in male smokers [8]. A recent Japanese study on comorbid lung cancer in patients with MACLD patients also showed a predominance of females, adenocarcinoma, and the nodular/bronchiectatic type of MACLD [18].
Considering the prevalence of lung cancer and MAC-positive cultures, Daley and Iseman [19] have speculated as to whether or not chronic inflammation caused by MAC infection leads to lung cancer, or if lung cancer allows the establishment of MAC infection. For the latter, MAC is believed to adhere to the non-ciliated epithelial cells in bronchioles at the onset of infection [20], with subsequent granuloma formation causing bronchial destruction and MACLD [21]. West and Dollery [22] have previously described variations in the ventilation-perfusion ratio between the upper and lower lungs and, by means of an analysis of the lung epithelial lining fluid using a bronchoscopy microsampling probe, revealed an increase in biomarkers such as carcinoembryonic antigen and cytokeratin fragment 19 concentrations in the fluid around lung cancer foci [23]. We can speculate that lung cancer allows the establishment of an exogenous MAC infection in the bronchioles around the lung cancer foci as a result of some unclear factors associated with the presence of lung cancer itself and/or other pre-existing lung diseases. Our finding that none of the 15 patients with lung cancer and non-MACLD progressed to MACLD may indicate an exogenous MAC infection under conditions suitable for transient infection.
The present study on lung cancer patients does not address lung cancer development associated with MAC infection, but many epidemiological studies have suggested that pulmonary tuberculosis increases the risk of lung cancer [24]. In a pathological study reported in 1939, Friedrich [25] first described a lung cancer that developed from a tuberculous scar, and the presence of scar carcinoma caused by tuberculosis has been historically recognized [26]. The development of lung cancer in NTMLD patients has not been reported in epidemiological studies. However, previous Japanese studies have reported that NTMLD/MACLD and lung cancer were likely to exist in the same lobe [9, 18] and often coexist in the same lesion [27]. The present study also demonstrated that for most of the cases with comorbid MACLD and lung cancer, the two diseases existed in the same lobe. In another study, analysis of the epithelial lining fluid revealed that the inflammatory reaction caused by MAC might spread to an unaffected area other than the original MAC-infected area [28]. Furthermore, attention has been paid to the Mendelian susceptibility to mycobacterial diseases, such as interferon gamma receptor deficiencies and impaired interleukin-2 production, although no data were presented here regarding this [29].
MACLD is a disease with a very long clinical course, and we must keep in mind that chronic inflammation caused by long-term MAC infection may exert some influence on cancer development.
Study Limitations
The present study had some limitations that are inherent because of the retrospective study design, the limited number of MAC-positive patients with lung cancer detected using bronchoscopy, and the limited patient data available in the medical records. In addition, there was a large population imbalance for the comparisons between MAC-positive/other NTM-negative (n = 25) and MAC-negative/other NTM-negative (n = 1,223) lung cancer patients. Because of this bias, the present data may not be sufficient to definitively elucidate MAC-positivity in patients with lung cancer. Larger epidemiological cohort studies and detailed clinicopathological studies may be required to clarify the relationship between lung cancer and MACLD/MAC infection.
CONCLUSION
The present study demonstrated an association between MAC infection and the presence of lung cancer. Female sex and advanced age were associated with MAC infection, corroborating previous studies. Lung cancer characteristics, including histological type, location, grade, and clinical stage, were not found to be associated with MAC infection.
ABBREVIATIONS
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

