All published articles of this journal are available on ScienceDirect.

Ethnic Variance in Prevalence of COPD among Smokers in a Real World Setting
Authors Info & Affiliations
Abstract
Introduction:
Chronic Obstructive Pulmonary Disease (COPD) is characterized by persistent and progressive airflow limitation generally caused by prolonged cigarette smoking. Ethnic differences have been reported regarding COPD risk from smoking. The purpose of this study was to compare COPD prevalence in Hispanic and Caucasian smokers in a real-world setting. We studied consecutive patients referred to the community-based pulmonary practice. Hispanic and Caucasian smokers were included in the study.
Methods:
The clinical diagnosis of COPD was recorded from the chart. COPD was defined by PFT using GOLD criteria. Exclusion criteria were other ethnicities, non-smokers, and patients with a history of asthma /other pulmonary conditions. We reviewed a total of 1,313 consecutive PFTs of which 797 patients met our inclusion criteria.
Results and Discussion:
The prevalence of COPD among Hispanics was found to be lower by both clinical diagnosis as well as by spirometry compared to Caucasians (41.6% vs 54.2%). In Hispanics, clinical diagnosis was 91% higher by PFT, whereas for Caucasians, it was 6% lower. The odds of developing COPD (diagnosed based on FEV1/FVC ratio <70%) in the Caucasians are 4.1 times higher than Hispanics (Odds Ratio: 4.1; 95%CI: 2.8-5.9). Hispanic smokers have a lower prevalence of COPD both by the clinical diagnosis as well as by PFT. There is a significant disconnection between clinical and PFT diagnosis of COPD in Hispanic patients.
Conclusion:
The genetic basis of lower COPD risk and prevalence in Hispanics needs to be better understood. Spirometry threshold criteria for confirming a diagnosis of COPD may need to be modified based on ethnicity in clinical practice.
1. INTRODUCTION
Chronic Obstructive Pulmonary Disease (COPD) is a common respiratory condition characterized by airflow limitation [1, 2]. It affects more than 5 percent of the population and is associated with high morbidity and mortality [3]. It is the major cause of death from chronic disease in the United States, having one of the highest rates of smokers, killing more than 120,000 individuals each year [4]. Ethnic differences have been previously reported in COPD prevalence amongst Hispanics, African Americans, and Asians [5-8]. Ethnic differences have also been noted in respiratory impairment [9]. A better understanding of ethnic differences in disease burden and disease susceptibility will enable us to target health inequalities and improve our understanding of disease pathogenesis.
The diagnosis of COPD is made on clinical grounds but needs to be confirmed by the use of spirometry, and a post-bronchodilator FEV1/FVC ratio of <0.7 has been recommended as the criteria to define the disease [10]. The purpose of our study was to assess the influence of ethnicity on the prevalence of COPD in a cohort of Hispanic and Caucasian smokers both in terms of the clinical diagnosis, as well as spirometry data, using the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria. We also wanted to examine the influence of ethnicity on spirometry values and the diagnosis of COPD in this population.
2. MATERIALS AND METHODS
This was a retrospective chart review of consecutive patients referred to a PFT lab in a community-based pulmonary practice. Inclusion criteria for entry into the current analysis were self-identified Hispanic and Caucasian patients, with self-reported smoking history, with symptoms of cough and/or dyspnea. Subjects were excluded from the review if they reported any other ethnicities or where ethnicities were not stated, non-smokers, any history of asthma / other known pulmonary conditions. Study participants’ data were anonymized before the analysis to assure patient confidentiality.
Spirometry, lung volume and diffusing capacity of carbon monoxide (DLCO) measurements were performed on all patients in accordance with the standard American Thoracic Society (ATS) guidelines [11] with pre- as well as post-bronchodilator measurements. COPD was defined according to the GOLD criteria, i.e. post-bronchodilator (BD) FEV1/FVC < 0.70. Clinical diagnosis of COPD was recorded from the chart based on physician (pulmonary specialist) diagnosis.
The prevalence of COPD was defined as the number of study participants with a current diagnosis of COPD (based on GOLD criteria or clinical diagnosis) divided by the total number of study participants.
Because this study involved only a retrospective chart review, it did not require approval from an ethics committee. All the categorical variables were expressed as percentages and continuous variables were expressed as mean and Standard Deviation (SD). The statistical difference in the categorical variables was tested using the χ2 test and continuous variables using the student t-test. A multiple regression model was constructed to identify independent risk factors for COPD diagnosis. Independent variables were sex, age, Body Mass Index (BMI), and respiratory symptoms (dyspnea, cough), with COPD diagnosis being the dependent variable. Odds ratios were presented with 95% Confidence Intervals (CI). P values < 0.05 were considered statistically significant.
3. RESULTS
This study included participants registered in the PFT lab between March 2018 and January 2020. We reviewed a total of 1,313 consecutive samples from the PFTs lab. Of which 797 participants met our inclusion criteria. The baseline demographic characteristics of all the study participants and the ethnic differences are shown in Table 1. Caucasians were slightly older and had a lower BMI, while the male gender was more prevalent in Hispanics.
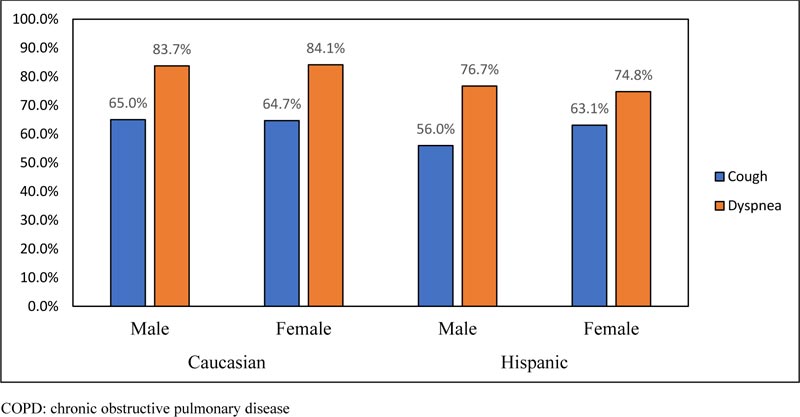
In terms of symptoms, there was a high prevalence of both dyspnea and cough in the cohort, however, these symptoms were more prevalent in Caucasian patients. Men reported a higher proportion of cough and dyspnea than women in both the ethnic groups (Fig. 1-2). The prevalence of COPD using clinical criteria was greater in Caucasian patients (54.2%) compared to Hispanics (41.6%).
When we examined the prevalence of COPD using PFT based on GOLD criteria, we found a marked difference in the prevalence of COPD, being far greater in the Caucasians than in Hispanics with the values of 55.1% and 21%, respectively. (Table 2). No gender difference was observed in the prevalence of COPD among Caucasians and Hispanics.
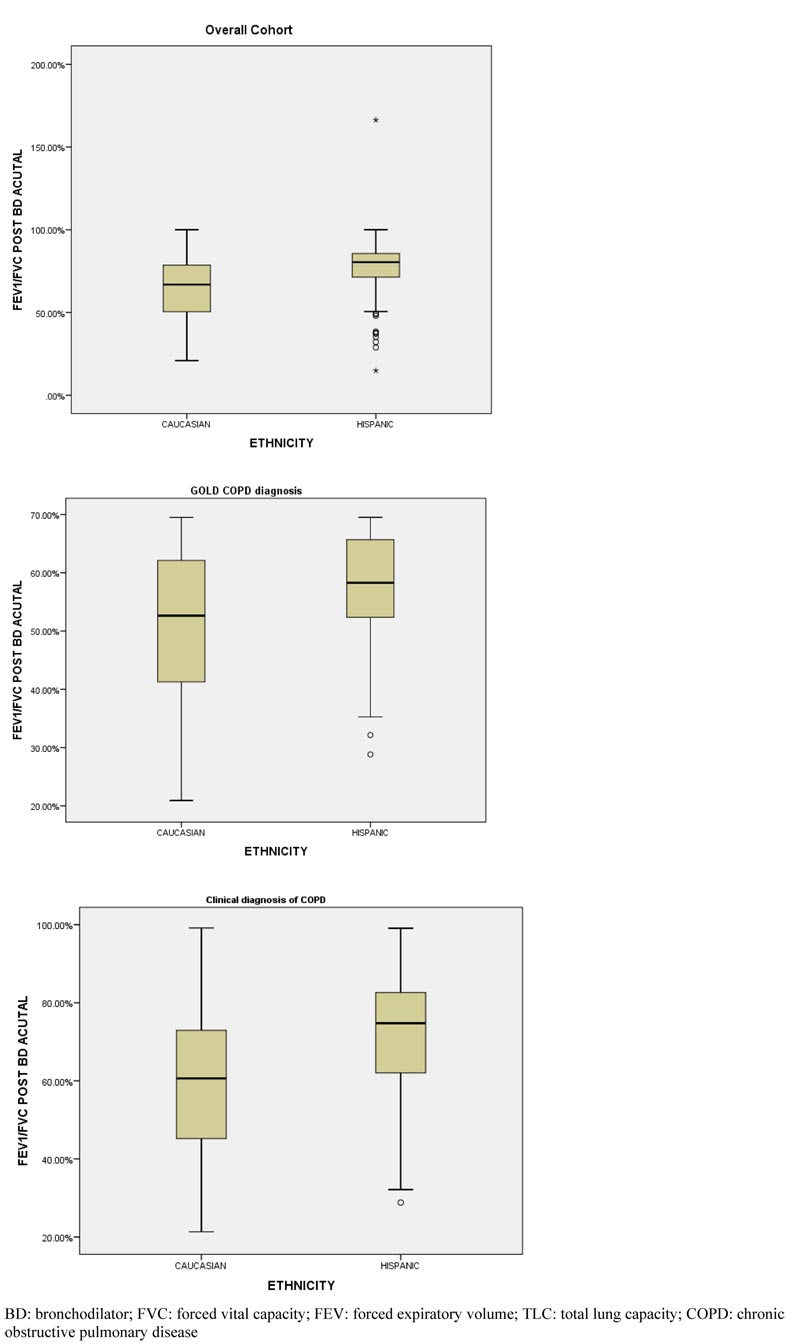
We also looked at ethnic differences in terms of full PFT results, including lung volumes and DLCO, in smokers with COPD based on clinical diagnosis and PFT confirmation of COPD based on GOLD criteria (Table 3). A total of 295 Caucasians and 55 Hispanics were found to be prevalent with COPD using GOLD criteria. Among them, 80 (27.1%) Caucasians had FEV1 Post BD % change of >12% compared to 9 (16.4%) in the Hispanics (Table 3). Boxplot showing the distribution of absolute values of FEV1/FVC post-BD among the ethnic groups is shown in Fig. (1). The absolute values of FEV1/FVC post-BD significantly differed among the two ethnic groups.
| Variables |
Caucasian (n=535) |
Hispanic (n=262) |
p-value |
|---|---|---|---|
| Male, n (%) | 283 (52.9%) | 159 (60.7%) | 0.038 |
| Age (in years) (Mean ± SD) | 69.26 ± 10.51 | 67.27 ± 12.33 | 0.018 |
| BMI (Mean ± SD) | 30.58 ± 8.1 | 32.78 ± 7.68 | 0.000 |
| COPD Diagnosis Criteria |
Caucasian (n=535) |
Hispanic (n=262) |
Total (n=797) |
p-value |
|---|---|---|---|---|
| GOLD Criteria | 295 (55.1%) | 55 (21.0%) | 350 (43.9%) | 0.000 |
| Clinical Diagnosis (Physician Diagnosed) | 290 (54.2%) | 109 (41.6%) | 399 (50.1%) | 0.001 |
| - | Clinician Diagnosis | GOLD Criteria | ||
|---|---|---|---|---|
| Caucasian (n=290) | Hispanic (n=109) | Caucasian (N=295) | Hispanic (N=55) |
|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| FVC pre-BD Actual | 2.49 ± 1.00 | 2.38 ± 0.80 | 2.49 ± 1.02 | 2.40 ± 0.80 |
| FVC post-BD Actual | 2.59 ± 1.04 | 2.45 ± 0.79 | 2.64 ± 1.05 | 2.53 ± 0.76 |
| FEV1 pre-BD Actual | 1.47 ± 0.76* | 1.67 ± 0.64* | 1.28 ± 0.64 | 1.40 ± 0.55 |
| FEV1 post-BD Actual | 1.54 ± 0.78* | 1.73 ± 0.64* | 1.36 ± 0.66 | 1.45 ± 0.52 |
| TLC Actual | 5.34 ± 1.41* | 4.83 ± 1.23* | 5.59 ± 1.49 | 5.44 ± 1.08 |
| DLCO Actual | 15.92 ± 6.54 | 16.51 ± 5.84 | 14.43 ± 5.89 | 14.60 ± 5.54 |
| FEV1 post-BD % Change | 5.76% ± 11.62% | 4.64% ± 9.55% | 7.2% ± 11.4% | 5.4% ± 11.2% |
| FEV1 post-BD % Change (Reversible)^ | 62 (21.4%) | 18 (16.5%) | 80 (27.1%) | 9 (16.4%) |
After adjustment for covariates (age, sex, and BMI), Caucasian ethnicity was significantly associated with a significant odds of airflow obstruction using the definition of FEV1/FVC ratio <70% (adjusted odds ratio: 4.096; (95% CI: 2.808-5.974) (Table 4). There was no significant difference in the risk of cough and dyspnea between the two ethnic groups in the statistical model.
| Outcomes | Unadjusted analysis | Adjusted analysis † | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% C.I. | p-value | Odds Ratio | 95% C.I. | p-value | |
| COPD (by GOLD) | 4.626 | 3.284-6.517 | 0.000 | 4.096 | 2.808-5.974 | 0.000 |
| COPD (Clinical) | 1.661 | 1.232-2.240 | 0.001 | 1.057 | 0.756-1.477 | 0.747 |
| Cough | 1.294 | 0.956-1.753 | 0.095 | 1.176 | 0.850-1.627 | 0.327 |
| Dyspnea | 1.653 | 1.147-2.382 | 0.007 | 1.355 | 0.914-2.007 | 0.130 |
| Ethnicity | GOLD Criteria | Cramer's V Correlation Coefficient |
p-value | |||
|---|---|---|---|---|---|---|
| Yes | No | |||||
| Hispanic | Clinical diagnosis of COPD | Yes | 39 | 70 | 0.306 | 0.000 |
| No | 16 | 137 | ||||
| Caucasian | Clinical diagnosis of COPD | Yes | 199 | 91 | 0.295 | 0.000 |
| No | 96 | 149 | ||||
Ethnic differences and correlation of COPD diagnosis using GOLD criteria and clinical diagnosis are presented in Table 5. A statistically significant difference was observed among the ethnic groups while using the GOLD criteria and clinical diagnosis in the study population.
4. DISCUSSION
In the present study, COPD prevalence was significantly higher among the Caucasians as observed by both clinical diagnoses as well as GOLD criteria based on spirometry. The odds of developing COPD (based on GOLD criteria) in Caucasians are 4.1 times higher than Hispanics. Hispanic smokers have a lower prevalence of COPD as observed by both the clinical diagnosis as well as by PFT. There was a significant difference between clinical and PFT diagnosis of COPD in Hispanic patients. In Hispanics, the clinical diagnosis by the physician was 91% higher than by spirometry, whereas for Caucasians, it was 6% lower. To our knowledge, this is the first study demonstrating a significant influence of ethnicity on the difference between clinical diagnosis and PFT confirmation in Hispanic patients compared to Caucasians.
Ethnic variance in COPD has previously been well described in the literature [5, 6, 12]. In a study by Martin et al. South Asian and black populations reported less severe breathlessness symptoms than their white counterparts [6]. Gilkes et al. found that black people in London were half as likely as whites to have COPD after adjusting for lower smoking rates in blacks, either due to ethnic differences in the way cigarettes were smoked or ethnic differences in susceptibility to COPD [12]. Similar differences have also been reported in Hispanic populations [8]. Sood et al. found that Hispanic female smokers in the New Mexico-based cohort had a lower risk of airflow obstruction and better lung function than Non-Hispanic White (NHW) female smokers [8]. The same group also reported new Mexican Hispanic smokers to have lower odds of COPD and less decline in lung function than the Non-Hispanic Whites [7].
In our study, Caucasians reported a higher proportion of cough and dyspnea compared to Hispanics. This could suggest that Hispanics have better tolerance in symptoms or milder COPD than Caucasians.
There were differences in age, with Caucasians being slightly older; however, the difference was small and likely did not contribute significantly to the ethnic difference in COPD. BMI causes a loss of expiratory reserve volume, which in turn causes an increase in the FEV1/FVC ratio. In our study, BMI in Hispanics was higher, and if anything, this may predispose them to more airflow limitation; however, this does not seem to have impacted their risk for COPD.
Our results are consistent with prior studies on the lower incidence of COPD in Hispanics and this is confirmed by the use of spirometry using GOLD criteria for COPD. Interestingly, the differences are more pronounced when compared to the clinical diagnosis of COPD.
Findings from this study indicate the likelihood of genetic factors that confer lower susceptibility to COPD among Hispanic smokers, as has been suggested in previous studies. There is also a possibility of dietary factors playing a protective role. Mortality from COPD has been found to be the lowest in Hispanic subjects, an observation described as the “Hispanic paradox”; a diet high rich in legumes has been speculated to confer a protective effect on COPD [13]. Significant ethnic differences in symptom descriptors have been previously described, which showed that Hispanic-Mexican Americans used both upper and lower airway ethnic word descriptors compared to Whites who used only lower airway descriptors [14]. This suggests that there may be a significant burden of COPD symptoms in Hispanics which may not get addressed using standard disease definition criteria for COPD. There is significant inconsistency in reckoning the influence of ethnicity while interpreting spirometry [15]. A Joint Working Party of the American Thoracic Society/European Respiratory Society (ATS/EAS) recommends the use of race- and ethnic-specific reference values when available. Alternatively, they recommend correction factors [16], however, these are not routinely or consistently followed [17].
The strengths of this study include the focus on the smokers and ethnic differences among them. The high levels of self-reported ethnicity in our study population enabled a robust estimation of the prevalence of COPD using three different criteria and helped in drawing a comparison among Caucasians and Hispanics. We also performed complete PFTs in a large group of people to enable more precise comparisons of pulmonary physiology. There are significant limitations to the study. The study was done in a PFT lab and hence selected patients who were already symptomatic or where a PFT test was not indicated. It was not a population-based cross-sectional survey. There was also a significant difference in the number of Caucasians >vs. Hispanics, which may have contributed to an element of bias in measuring COPD prevalence. Clinical diagnosis of COPD was based on the chart review, so we did not have a standardized approach to defining clinical COPD which may have affected the data quality. While we were unable to determine if any study participants were having an ongoing exacerbation, we do not feel this may be a significant factor, as pulmonary specialists would typically not order PFT in that scenario. We also did not have detailed ethnic data in terms of subtypes of ancestry in Hispanic ethnicity, nor did we have details of other comorbidities which could influence the disease pathology, and hence this could not be analysed.
CONCLUSION
In summary, this study adds to the body of literature that there exist strong ethnic influences on disease expression in COPD from smoking and Hispanics have a markedly low rate of COPD based on both clinical diagnosis as well as spirometry, compared to Caucasians. However, the differences in symptom profile are not as marked and PFT diagnosis confirms COPD in only 50% of clinically diagnosed COPD in Hispanics, which suggests that the use of standard spirometry criteria may significantly underdiagnose COPD. This has important implications for screening COPD and appropriate long-term disease management in Hispanic populations.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

