All published articles of this journal are available on ScienceDirect.

The Changing Pattern of Non-Small Cell Lung Cancer Between the 90th and 2000th Decades§
Authors Info & Affiliations
Abstract
Background:
In Europe, approximately 381,500 patients are diagnosed with non-small cell lung cancer (NSCLC) every year. The aim of this study is to analyse the changes in diagnosis, treatment and evolution during the last two decades, using data from a hospital registry.
Material and Methods:
Patients diagnosed with NSCLC at the Corporació Sanitària Parc Taulí-Sabadell (Catalonia, Spain) during the periods 1990-1997 (n=748) and 2003-2005 (n=311) were included. The hospital tumour registry was used for prospective data collection.
Results:
Our series shows a significant increase in women diagnosed with NSCLC (6% vs 10.3%; p 0.01) in the latter period; the incidence of adenocarcinomas increased by 20% (31% vs 51.1%), whereas that of squamous cell carcinomas fell (51.3% vs 32.5%; p<0.001). The proportion of patients receiving active treatment also increased significantly, from 56.6% to 76.5% (p<0.001). Disease stage at diagnosis and the number of patients treated by radical surgical resection remained unchanged. Among the favourable independent prognostic factors for survival were: gender (women), age less than 70 years old, Karnofsky index ≥70%, early stage at diagnosis, treatment with chemotherapy, and being diagnosed in the latter period 2003-2005 (HR 0.67). Over this 10-year period, absolute gain in mean survival in our series was 115 days.
Conclusions:
The absolute gain in mean survival in NSCLC patients in the period studied was 3.8 months, with a 6.75% increase in 5-year survival. Hospital registry data may help the correct assessment of epidemiological changes and the real effectiveness of treatments, which are sometimes overestimated in clinical trials.
INTRODUCTION
Cancer remains a high-priority public health problem. Worldwide prevalence of cancer is around 3% and reaches 15% at advanced ages [1,2]. Lung and prostate are the leading cancer sites among men, and lung is the fourth most common among women [3]. In the European Union 381,500 new cases of lung cancer are diagnosed every year, with 341, 800 deaths [4]. Survival rates are low: 30% at one year and 10% at five years [5, 6]. Over 16,600 cases of lung cancer are diagnosed in Spain every year, accounting for the greatest number of cancer deaths [7, 8].
Non-small cell lung cancer (NSCLC) is the most common histological type, accounting for 80% of all lung cancers. Treatment is determined according to the stage of the disease; surgery remains essential in the early stages, whereas multimodal treatment with chemotherapy, radiotherapy and sometimes surgery is favoured at locally advanced stages. Meta-analyses and clinical trials show an increase in survival and quality of life with systemic palliative chemotherapy for disseminated stages. Despite the positive results in survival obtained in patients in clinical trials, the real impact on the general population diagnosed with NSCLC seems minor and overall prognosis remains poor [5,6,9,10].
The aim of this study was to describe and compare the epidemiological, therapeutic and prognostic characteristics of patients diagnosed with NSCLC in a north-eastern Spanish hospital in the last two decades. The study used our centre’s hospital-based cancer registry, an invaluable source for assessing the epidemiological factors associated with cancer, as well as prognostic variables and outcomes [11].
PATIENTS AND METHODS
Study design:
Single-centre, prospective, naturalistic, open-label, observational study.
Setting:
Oncology service of the Corporació Sanitària Parc Taulí (CSPT), a university hospital affiliated to the Universitat Autònoma de Barcelona (UAB) with high technological standards and a catchment population of over 400,000 inhabitants.
Sample size:
As large cell carcinoma is the NSCLC with the lowest prevalence (around 10%), for statistical evaluation we needed a minimum of 30 patients in this group. We therefore required at least 300 patients (n ≥ 300) in each period.
Patient Recruitment:
The hospital thoracic tumour registry was used to select all the patients with cytologically or histologically-confirmed NSCLC diagnosed from January 1990 to December 1997 and from January 2003 to December 2005. Patients were included in the analysis until death or last follow-up.
Study Protocol
Registry variables:
age, sex, histologic subtype and grade, tumour stage according to UICC-TNM 5th ed. classification [12], Karnofsky index, type of treatment received and death.
Patients diagnosed in the first period were reclassified according to the 5th UICC-TNM ed. classification. Both Karnofsky index and age were categorised with the usual cut-off values. All the variables were recorded prospectively except the date of death, which was recorded retrospectively from the hospital attendance register and the death records of the Health Department of Catalonia.
Intervention:
All patients were discussed by a multidisciplinary institutional committee including the various specialists involved: pathologists, medical oncologists, radiotherapists, pulmonologists, thoracic surgeons and radiologists. Therapeutic decisions were taken by consensus of the committee and based on the approved clinical guidelines at each moment.
Informed consent:
The Internal Review Board (IRB) of the Corporació Sanitària Parc Taulí was informed of the data collection procedure. Informed consent was considered unnecessary because the patients received the habitual protocol of treatment, no confidential data were collected, and the statistical analyses remained private.
Statistical Analysis
Results are expressed as median (range) and percentages. Univariate analysis was performed using the Chi-square test to assess associations between categorical variables, and the Student ‘t’ test to analyse quantitative variables. Survival curves were estimated using Kaplan Meier methods, and the log-rank test was used to compare survival between groups of patients. Multivariate analysis using the Cox proportional hazards model was used to identify independent prognostic factors for survival. Adjustments were made for co-variables that were clinically relevant or significant in bivariate study. Statistical tests were considered significant at p<0.05 (two-sided). Survival was calculated from date of diagnosis. Statistical analysis was performed using SPSS® 17.0 and Stata® v10.0 packages.
RESULTS
A total of 1,059 patients diagnosed with NSCLC were assessed during the two study periods: 748 between 1990 and 1997 and 311 between 2003 and 2005. Median follow-up was 13.5 years (3.4-19.5): 14.9 years (11.6-19.5) for patients diagnosed during the first period and 5.3 years (3.4-7.3) for those diagnosed during the second period.
General Data
Our series included 982 men (92.7%) and 77 women (7.3%), with a median age at diagnosis of 67.5 years (range 32-95). Some aspects of NSCLC diagnosed during the two periods showed major changes (Table 1). The percentage of women diagnosed rose from 6% in the first period to 10.3% in the second (p=0.01); the male-to-female ratio fell from 16:1 in the first period to 9:1 in the second. Furthermore, the proportions of squamous cell carcinoma and adenocarcinoma changed dramatically between periods. Squamous cell histology was predominant in the 1990s, accounting for 51.3% of cases, while adenocarcinoma was diagnosed in 31%; in the last decade these figures reversed, with 32.5% (p<0.001) of lung cancers diagnosed being squamous cell carcinomas and 51.1% adenocarcinomas (p<0.001). Another relevant issue is the type of treatment received by patients. In the first study period, 44.4% of patients received no oncological treatment, whereas between 2003 and 2005 only 23.5% (p<0.001) received supportive care alone. The number of patients receiving chemotherapy doubled (31.4% vs 59.8%; p<0.001), although the percentage of patients who underwent surgery did not change. No changes were observed regarding age of diagnosis or initial tumour stage, as the rate of patients diagnosed at locally advanced or disseminated stages remained around 75%.
Comparison of General Data Between the Two Periods
| 1990-1997 (n =748) | 2003-2005 (n=311) | p Value | |
|---|---|---|---|
|
|
|||
| Age (Median; range) | 67 (32-91) | 68 (33-95) | ns |
|
|
|||
| Sex | |||
| Male | 703 (94%) | 279 (89.7%) | p 0.014 |
| Female | 45 (6%) | 32 (10.3%) | |
|
|
|||
| Histology | |||
| Squamous cell Ca | 384 (51.3%) | 101 (32.5%) | p<0.001 |
| Adenocarcinoma | 232 (31%) | 159 (51.1%) | p<0.001 |
| L. Cell/Undifferentiated | 106 (14.2%) | 41 (13.2%) | ns |
| Unknown | 26 (3.5%) | 10 (3.2%) | ns |
|
|
|||
| Differentiation | |||
| Grade I | 16 (2.1%) | 9 (2.9%) | ns |
| Grade II | 116 (15.5%) | 38 (12.2%) | ns |
| Grade III | 233 (31.1%) | 135 (43.4%) | p<0.001 |
| Unknown | 383 (51.2%) | 129(41.5%) | p 0.004 |
|
|
|||
| Stage | |||
| Ia | 43 (5.7%) | 31 (10%) | ns |
| Ib | 70 (9.4%) | 21 (6.8%) | |
| IIa | 0 | 8 (2.6%) | |
| IIb | 42 (5.6%) | 18 (5.8%) | |
| IIIa | 44 (5.9%) | 28 (9%) | |
| IIIb | 155 (20.7%) | 86 (27.7%) | |
| IV | 276 (36.9%) | 116 (37.3%) | |
| Unknown | 118 (15.8%) | 3 (1%) | |
|
|
|||
| Treatment | |||
| Supportive care | 332 (44.4%) | 73 (23.5%) | p<0.001 |
| Surgery | 167 (22.3%) | 63 (20.2%) | ns |
| Chemotherapy | 235 (31.4%) | 186 (59.8%) | p<0.001 |
| Radiotherapy | 151 (20.2%) | 120 (38.7%) | p<0.001 |
Cox Multivariate Regression Model
| Variable | Hazard Ratio | 95% CI | p Value |
|---|---|---|---|
|
|
|||
| Age | -- | ||
| ≤70 | 1c | 1.039 to 1.430 | -- |
| >70 | 1.219 | 0.015 | |
|
|
|||
| Sex | |||
| Female | 1c | -- | -- |
| Male | 1.377 | 1.041 to 1.821 | 0.025 |
|
|
|||
| Karnofsky Index | |||
| <70 | 1c | -- | -- |
| ³70 | 0.439 | 0.361 to 0.534 | <0.001 |
|
|
|||
| Histology | |||
| Squamous cell Ca | 1c | -- | -- |
| Adenocarcinoma | 1.058 | 0.899 to 1.245 | 0.499 |
| Large cell/Undifferentiated | 1.240 | 1.000 to 1.537 | 0.05 |
|
|
|||
| Stage | |||
| Ia-IIb | 1c | -- | -- |
| IIIa-IIIb | 2.550 | 2.058 to 3.158 | <0.001 |
| IV | 5.283 | 4.281 to 6.520 | <0.001 |
|
|
|||
| Chemotherapy | |||
| No | 1c | -- | -- |
| Yes | 0.706 | 0.591 to 0,843 | <0.001 |
|
|
|||
| Period | |||
| 1990-97 | 1c | -- | -- |
| 2003-05 | 0.670 | 0.563 to 0.797 | <.001 |
Cases available in analysis: 865 (81.2%).
c Reference category.
Survival
Median survival of the total group of patients studied (n=1,059) was 233 days (7.7 months). One year after diagnosis, practically two thirds of the patients had died. These figures improved overall during this 10-year period; the data collected showed a 12.9% increase in the one-year survival rate (32.6% vs 45.5%) and a 6.75% increase at five years (8% vs 14.75%). In absolute terms, the median survival of patients diagnosed during the first period was 205 days (6.7 months) with an increase of 115 days (3.8 months) in the second period. Modest to substantial improvements in survival were observed for all stages in the second time period (Table 2). Fig. (1) shows the survival curve for the entire group and differences observed between the two periods.
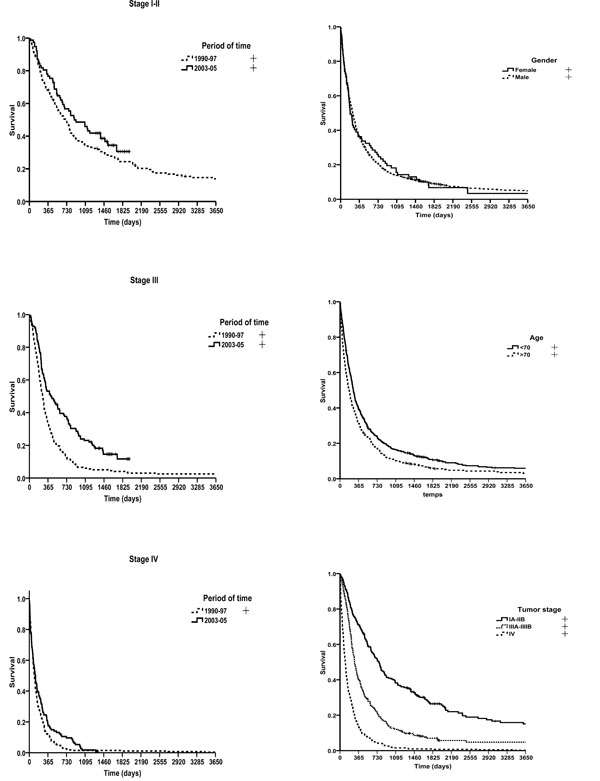
Overall survival and survival by period of diagnosis.
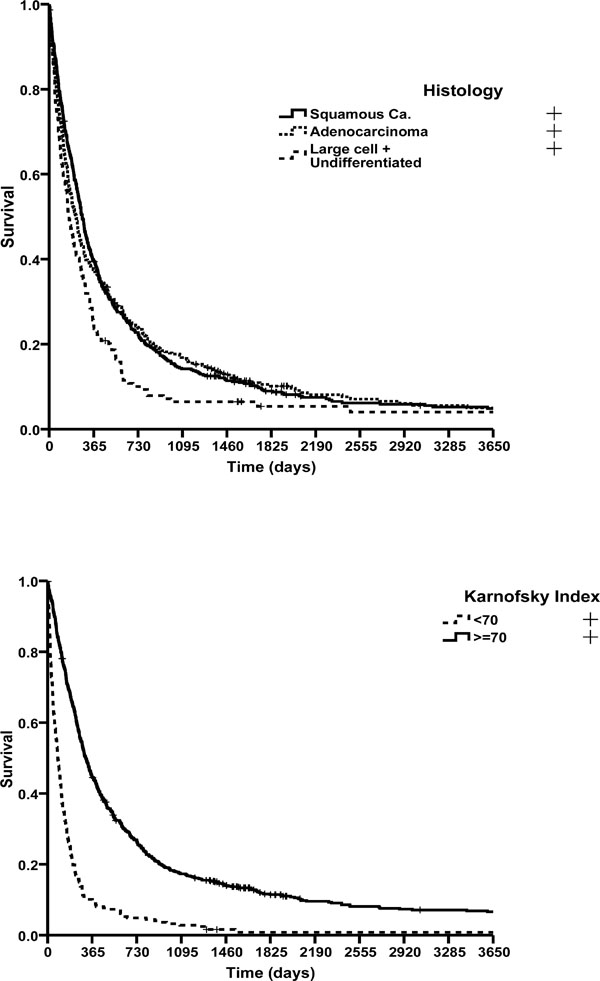
Survival curves by gender, age, tumour stage, histology and Karnofsky index.
Univariate analysis of survival.
Differences in survival were found in all diagnosed patients when comparing stages at diagnosis (p<0.001). Median survival was 765 days at initial stages (IA-IIB), and 286 days at locally advanced stages (IIIA and IIIB), falling to 103 days at advanced stages. Patients over 70 years of age at the time of diagnosis had a poorer prognosis, with a median survival of 181 days vs 261 days in patients of 70 years or younger (p<0.001). No differences were observed between sexes (p=0.96). Median survival was 314 days for patients with a good performance status at diagnosis (Karnofsky index ≥70) and only 84 days for those with a Karnofsky index <70 (p<0.001). The median survival time was 272 days for patients diagnosed with squamous cell carcinoma, 222 days in cases of adenocarcinoma and 156 days in cases of large cell/undifferentiated carcinomas (p=0.002) (Fig. 2). Likewise, median survival varied according to the histological differentiation of tumour: 524 days for well differentiated cancers (g1), 274 days for moderately differentiated ones (g2), and 248 days for poorly differentiated ones (g3), (p=0.3). Finally, patients treated with chemotherapy had a longer survival (328 days) than those who did not (155 days; p <0.001).
Multivariate analysis of survival.
Clinically relevant or statistically significant variables for univariate analysis were included in a multivariate Cox regression analysis. Sex, age, Karnofsky index, histology, stage, chemotherapy and period of diagnosis were identified as independent prognostic factors for survival (Table 3).
The analysis showed that males have a worse prognosis than females (HR 1.37; p=0.02) and that age over 70 years per se also worsened prognosis (HR 1.21; p=0.01). A good performance status at diagnosis with a Karnofsky index ≥70 was linked to better survival (HR 0.43; p<0.001). Histologically, only the subgroup of large cell or undifferentiated carcinomas presents a risk of death higher than the reference (in this case, squamous cell carcinomas - 1.24 times higher, p=0.05). One of the factors with the greatest impact on survival is the stage of the disease at diagnosis. Taking localised stages as a reference, the risk of death increased 2.5 times (p<0.001) when the disease was diagnosed at stage III, and up to 5.2 times (p<0.001) if diagnosed at stage IV. Administration of chemotherapy also lowers the risk of death (HR 0.7; p<0.001). Lastly, we observed that patients diagnosed with NSCLC during the second period (2003-2005) survived longer than those diagnosed during the first (HR 0.67; p<0.001).
DISCUSSION
Using data from patients diagnosed with NSCLC at our centre during the two periods 1990-1997 and 2003-2005, we assessed changes in epidemiology, characteristics of tumours, and treatments administered. We also analysed the differences in survival between the two groups.
Patients’ information was obtained from the hospital tumour registry, a reliable source that provides data on all variables. We compared these two time periods because treatments administered in each one were reasonably homogeneous, with no significant changes in the therapeutic approach inside each period. Although the number of patients included was higher in the first period, the sample size requirements were met. A meta-analysis published in 1995, demonstrating a significant but modest survival benefit of chemotherapy compared with supportive care alone in patients with advanced NSCLC [9], led to an important change in strategy and in the late 1990s combinations with newer third-generation cytotoxic drugs improved response rate and survival. In the last decade new drugs have been developed for specific biological pathways, offering increased specificity and reduced toxicity. Trial BR21, published in 2005, proved that erlotinib, an oral tyrosine kinase inhibitor for epidermal growth factor receptor, improved overall survival compared with placebo in previously treated patients with NCSLC [19]. Below we discuss the influence of the different treatments in the population analysed.
Our study detected a significant increase in the percentage of women diagnosed with lung cancer in recent years. The causal relationship with smoking is obvious and this upward trend is comparable to countries where women started smoking earlier, such as the United States. In fact, incidence and mortality rate for lung cancer amongst men has fallen, while it has increased for women [13]. According to data obtained from a National Health Survey performed in Spain in 1993, 44% of adult men smoked, compared with 20.8% of women; by 2006, tobacco consumption had dropped to 31.6% in men and increased to around 21.5% in women. Regarding survival rates according to sex, our study shows that men present a moderately worse prognosis than women, independent of other variables (HR 1.37). Other registries such as the SEER in the US [13] and others in Japan [14] have also found higher percentages of 5-year survival in women than in men (around 5%), and the Eurocare-4 project reported better prognosis for women in most cancers except for tumours of the biliary tract, larynx, and urinary bladder [6]. The excess risk of death for males is 1.05 (95% CI: 1.04, 1.05) [15]. The reasons why women have a better prognosis than men are unknown: comorbidity factors, biological advantages or cultural factors such as better compliance with treatment, follow-up and physicians’ indications have been suggested as possible causes [16].
Dramatic changes in the histology of non-small cell lung cancer have been recorded in the past two decades. The incidence of squamous cell carcinomas has decreased by 30%, while that of adenocarcinomas has risen in the US, Canada, Australia, the Netherlands and elsewhere. The SEER data in the US (2002-2006) [13] show that of all lung cancers, 14% correspond to small cell, 19.9% to squamous cell carcinomas, 36.9% to adenocarcinomas, 3.5% to large cell and 24.6% to other types. Similar trends have been observed in most developed countries. No such change had been noted in Spain in the year 2000 [17], but our series shows a striking change between our two time periods; the proportion of squamous cell carcinomas had fallen by 20% in the 2003-2005 period, whereas adenocarcinomas had increased by the same amount. The reasons for this change in the histopathology of NSCLC seem to be related to tobacco consumption, which causes 90% of diagnosed lung cancers. Changes in smoking habits, with Virginia tobacco gradually replacing dark tobacco and filtered cigarettes gradually replacing unfiltered ones, and changes in the composition of certain brands with a reduction in polycyclic aromatic hydrocarbons and an increase in N-nitrosamines seem to be the cause of this variation in the histopathology of lung cancer in such a short period [16, 17].
Therapeutic strategy also underwent a notable change during this time period. The results of comparative trials and meta-analyses performed in the mid-1990s argued in favour of the use of chemotherapy instead of supportive care and by the year 2000, the publication of trials with second-line antitumour treatments gave further support to the change in therapeutic approach [9,10,18,19]. Our study shows that over the two periods the proportions of chemotherapy and radiotherapy increased by 30% and 20% respectively, whereas surgery has remained stable. Fifteen years ago, 44.4% of patients in our series received only supportive care, but this figure dropped to 23% in 2003-2005. The use of oncological treatments in patients who performed well in the first trials increased survival by more than two months for both the first and the second line of treatment. The introduction of new target therapies seems to maintain this tendency.
Population- and hospital-based registries include many patients who would not have been included in clinical trials for personal or disease-related reasons. Thus, one should be cautious when extrapolating the results of clinical trials to the general population diagnosed with NSCLC. Further studies like this one are necessary to assess the real effectiveness of treatments and the evolution of cancer control measures, and are made far easier if a hospital-based registry is in place.
Our study shows that the difference in overall survival in the two periods of time was 115 days (3.8 months); 1-year survival increased from 32.6% to 45.5% and 5-year survival from 8% to 14.75%. These figures are comparable with those obtained in neighbouring countries. Eurocare-4 (1995-1999) [6] reported a 1-year survival of 36% and a 5-year survival of 12%. In Spain, Eurocare-4 showed survival rates at 1 and 5 years of 34.2 and 10.2% respectively. When reviewing the tendency towards increased survival in population registries, we observe that 5-year survival (e.g., in the United States) has risen from 13.8% in 1990 to 16.2% in 2000, which represents an increase of less than 2.5% in patients alive at 5 years [20].
Some limitations should be borne in mind when extrapolating our findings to other medical centres. The demographic, social and economic characteristics of the population should be taken into consideration, as should differences in accessibility and in the availability of technological resources at each hospital. The reference population of our sample was predominantly from the urban and industrial area of Barcelona. During the study period, patients’ fidelity to their reference hospital was high and the medical and surgical team remained stable. As this is a teaching hospital with extensive experience in treating such patients and promoting research, we consider that the data obtained in our study may be representative of other areas in Spain as well as neighbouring countries.
Another important limitation in our study is that the degree of tobacco consumption of patients is not reflected. This information was initially recorded as number of packet-cigarettes/day and then as packets/year, so it is difficult to compare the two periods.
Despite the advances in recent years, lung cancer remains the leading cause of cancer deaths. Treatments should be improved and primary prevention of smoking promoted to increase the modest survival benefits described. Hospital tumour registries provide very useful information to complement that obtained from experimental clinical research studies and population-based registries [6,13,14,21,22] and provide a broader picture of the trends in the control of malignant diseases.

