All published articles of this journal are available on ScienceDirect.

Tracheostomy-related Tracheal Tears in Pediatrics
Authors Info & Affiliations
Abstract
Introduction:
Tracheostomy-related tracheal tear is a serious complication that may follow surgical or percutaneous tracheostomy. Pediatric populations carry a higher risk because of anatomical differences. The aim of this article is to review this condition and to help in its diagnosis and management with the assistance of clinical and radiological findings.
Materials and Methods:
An English literature review was done using the terms pediatric, tracheostomy, tracheal tear and tracheostomy tube.
Result:
Two cases reported in the literature met the criteria to be included in the review.
Discussion:
Tracheostomy-related tracheal tear needs immediate diagnosis as it may lead to life-threatening outcomes, such as pneumothorax, respiratory distress, extensive subcutaneous emphysema and pneumomediastinum. Symptoms and complications of the tear may occur intraoperatively or postoperatively. Gold standard methods for diagnosis include flexible or rigid tracheobronchoscopy, which helps in determining the management plan. The treatment choices for iatrogenic tracheal tears depend on the tear site, size, and extension of the tear and patient’s hemodynamic status. Conservative management is sufficient for stable patients with small tears, whereas surgical management is essential for unstable patients and those with large or complicated tears.
Conclusion:
Tracheostomy-related tracheal tear is a serious rare complication. The pediatric age group carries a higher risk of the condition and its management, either conservative or surgical, depends on airway endoscopy findings and patient’s hemodynamic status.
1. INTRODUCTION
Tracheal tear is a rare but potentially fatal complication of thoracic or neck injuries, spontaneously or iatrogenically during intubation and, less commonly, bronchoscopy, surgical and percutaneous tracheostomy [1, 2]. The aim of this article is to review tracheostomy-related tracheal tear in pediatrics and help in its diagnosis and management with the assistance of clinical and radiological findings.
2. MATERIALS AND METHODS
An English literature review on PubMed, Ovid, Medline and Cochrane collaboration databases was done using the terms pediatric, tracheostomy, and tracheal tear. Inclusion criteria included patients below the age of 18 years and with tracheostomy-related tracheal tears. Exclusion criteria included patients above the age of 18 years and with other causes of tracheal tears other than tracheostomy.
3. RESULTS
Two patients reported only met the criteria to be included in the review; their data are presented in Table 1.
| Patient Data | Diagnosis | Management |
|---|---|---|
| Case 1: -Newborn with of Nager syndrome underwent tracheostomy. -Posterior tracheal tear occurred at the time of tracheostomy tube placement -Post operative, patient was difficult to ventilated and arrested |
After Patient stabilization, bedside tracheoscopy demonstrated a large membraneous tear in the posterior tracheal wall. | Conservative management involving advancing tracheostomy tube beyond the tear |
| Case 2: -18 y/o male underwent tracheostomy after a prolonged intubation -3 weeks post operative patient develop subcutaneous emphysema involving his upper torso, face, and neck along with volume loss noted on the mechanical ventilator and borderline hypoxemia. |
-CT revealed extensive soft tissue emphysema and tracheostomy tube was noted to perforate posterior tracheal wall into the posterior mediastinum. -Bronchoscopic evaluation, revealed false passage in posterior wall of mid trachea with distal tip of tracheostomy tube perforating tracheal wall. |
Conservative management include intubation with rigid bronchoscope followed by silicon stent |
4. DISCUSSION
In the pediatric population, intubation-related tracheal tear due to a large endotracheal size is the most common mechanism of airway injury, so the selection of appropriate tube size is essential [3, 4]. Furthermore, frequent manipulation of the tube without overinflation or deflation and intubation performed by inexperienced clinicians are common causes of tracheal tears [5].
Tracheostomy-related posterior tracheal tears occur infrequently and are less common than the intubation-related tracheal tear. They usually occur during tracheostomy placement either using cuffed tubes with overinflation of the cuff or during tracheostomy tube introducer insertion [6-8]. Tracheostomy-related tears are mainly located proximal to the carina and distal to the insertion point of the tracheostomy [3, 9]. Pediatric patients are at higher risk of iatrogenic tracheal tears than adults due to anatomical differences: weaker intercartilaginous membrane, higher cartilage elasticity, and smaller airway lumen. In addition, the mortality rate in pediatric patients after iatrogenic tracheal tears is as high as 75%, so the selection of the appropriate tube size is essential [3]. Short thick neck, kyphoscoliosis, and emergency cases with difficult intubation increase the risk of tracheal tears in pediatric patients [1, 7, 9].
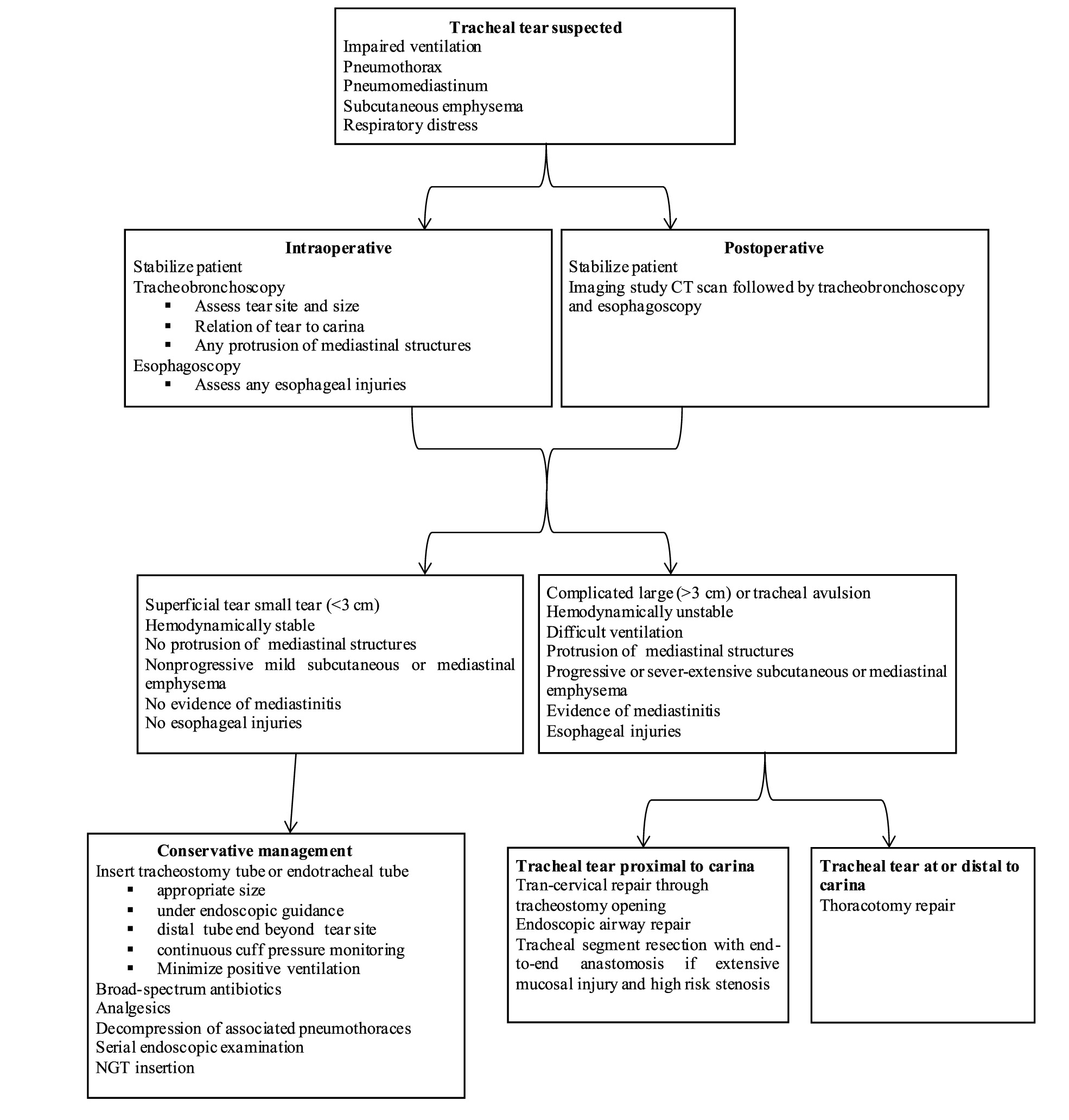
Iatrogenic tracheal tears may present immediately as impaired ventilation or later in the postoperative period with the complications of compressive pneumothorax, pneumomediastinum, or extensive subcutaneous emphysema, especially during retching or coughing or in mechanically ventilated patients [1, 10]. Furthermore, tracheobronchial tears can lead to many other complications, such as respiratory distress, mediastinitis, tracheal stenosis, recurrent nerve injury, fistula, and abscess. The gold standard methods for diagnosis are flexible or rigid tracheobronchoscopy, which help determine the site, extension, and location of the tear with respect to the carina. Imaging studies, such as computed tomography (CT), can help identify complications, such as pneumothorax, pneumonia, pneumomediastinum, and mediastinitis. Chest and lateral neck radiographs are helpful, but they have a false negative rate reaching 10% [1, 2, 5, 9, 10]. In addition, esophagoscopy is essential to rule out esophageal injuries [3, 10]. In 88% of cases, tears are diagnosed intraoperatively because of emphysema in the mediastinum or impaired ventilation [11].
Treatment can be conservative or surgical. Conservative treatment is indicated for mechanically ventilated patients and hemodynamically stable patients with uncomplicated and small [<3 cm] tears, no protrusion of mediastinal structures into the tracheal lumen, and only mild emphysema. Conservative treatment includes the insertion of longer/adjustable-length tracheostomy tubes or endotracheal tube, preferably under endoscopic guidance with an appropriate tube size, which is placed distal to the tear site with continuous cuff pressure measurement. If the tear is close to the carina, positioning the cuff distal to the tracheal tear is challenging, so tube placement should be performed under endoscopic guidance to ensure proper tube placement, along with continuous cuff pressure measurement to avoid tear enlargement [1, 5, 10,12-14]. Fur-thermore, the type of mechanical ventilation is important as positive pressure ventilation can exacerbate the injury. On the other hand, spontaneous ventilation helps the tear to collapse, thus supporting tear healing. All this should be done under the cover of a broad-spectrum antibiotic to reduce the risk of infection [1, 3, 10]. Surgical treatment is preferred for patients with larger complicated tears, tracheal avulsion, extensive emphysema, and those who are unstable during ventilation.. Surgical repair should be performed as soon as possible to decrease the risk of complications. The choice of surgical approach should be guided by the anatomical site of the tear. Using the tracheostomy opening is highly recommended because the incision already exists, and the tear is almost always proximal to the carina and rarely extends beyond it [1]. Deganello et al. described the surgical repair of a large proximal tracheal tear that ended above the carina in an adult patient through an extended tracheotomy opening technique with interrupted sutures using a thoracoscopic needle holder [1]. Welter et al. described a repair of a similar tear with no surgical access using an optical needle holder with interrupted sutures through rigid bronchoscopy [13]. Chaaban et al. treated a large tear in a surgically unfit tracheostomized adult patient using a customized silicone stent, which was inserted under bronchoscopy guidance to bridge the tear end. Then, at the level of the tracheostomy site, an anterior window was made in the stent to insert the tracheostomy tube through the stent [14]. If the tear extends up to the bronchial tree, thoracotomy is required. Tears involving the carina, right bronchial tree, and proximal region of the left main bronchus necessitate right thoracotomy. Left thoracotomy is required if the injuries lie in the left main bronchus near the lung hilum and left bronchial tree [5]. If significant tracheal mucosa injury and concern of stenosis are present, tracheal segment resection with end-to-end anastomosis may be performed. In addition, sealing the tear at the anterior esophageal wall can help secure the tear. After the repair of the tear, a soft non-cuffed tube should be used. If a cuffed tube is used, the cuff pressure needs to be monitored. To decrease peristaltic movement, a nasogastric tube should be inserted for at least 1 week. For both surgical and nonsurgical treatment, multiple follow-up chest and lateral neck radiography are needed, as well as regular serial endoscopic including daily bedside fiberoptic endoscopy and operative bronchoscopy after few days. During the assessment, the endotracheal or tracheostomy tube should be carefully retracted to check for healing, proper tube placement at a suitable level, and evidence of stenosis or tracheoesophageal fistula [1, 9, 11]. An algorithmic approach for diagnosis and treatment of tracheostomyrelated tracheal tears is illustrated in Fig. (1).
CONCLUSION
Tracheostomy-related tracheal tear is a serious rare complication. The pediatric age group carries a higher risk of the condition and its management depends on airway endoscopy finding and patient’s hemodynamic status. Conservative management is sufficient for stable patients with small uncomplicated tears, whereas surgical management is essential for unstable patients and those with larger complicated tears. Tracheostomy-related tears are often proximal to the carina so the tracheostomy opening can be used during repair surgery. Thoracotomy is required if the tear involves the bronchial tree.
PRESENTATION
Article was presented as a poster at SENTAC and the Aerodigestive Society Combined Virtual meeting, United States of America, December 2020.
LIST OF ABBREVIATIONS
| CT | = Computed Tomography |
| USA | = United States of America |
AUTHORS’ CONTRIBUTION
Ali Alsudays and Mazyad Alenezi were involved in the data collection and writing of the initial manuscript. Sultan Alanazy contributed to data collection. Eman Almashharawi and Samir Bawazir revised the article.
CONSENT FOR PUBLICATION
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

