All published articles of this journal are available on ScienceDirect.

Impact of Blood Cultures on the Changes of Treatment in Hospitalized Patients with Community-Acquired Pneumonia
Authors Info & Affiliations
Abstract
Background:
Initial blood cultures (BCs) with severe community-acquired pneumonia (CAP) are warranted. However, other than severity, the specific contributing factors that affect the decision to change antimicrobial agents have not been evaluated previously.
Methods:
Consecutive adults with CAP hospitalized between January 2008 and December 2010 were assessed retrospectively. We enrolled those who were over 18 years old with typical symptoms of pneumonia and with an infiltrate consistent with pneumonia, from which 2 sets of BCs were obtained. Those who had been immunocompromised, hospitalized, or prescribed antibiotics in the past 30 days were excluded. We retrospectively assessed the factors contributing to the change in antimicrobial agents as well as the frequency of these changes in the enrolled patients based on the initial BC results.
Results:
In total, 793 patients with initial diagnosis of CAP were admitted; 399 met the inclusion criteria. Among them, 386 were made definitive diagnosis of CAP after admission (the remaining 13 were made alternative diagnosis [non-pneumonia illnesses]). BC results were positive in 17 (4.4%) out of 386 CAP patients, among whom antimicrobial therapy was changed based on the BC results in 8 (2.1%) (Pneumonia Severity Index [PSI] grade IV; 2, PSI grade V; 6). Alternative diagnosis after admission was contributing factors for changing antimicrobial agents based on the positive blood culture results.
Conclusions:
The use of BCs should be limited to patients with very severe cases. It would be helpful to find alternative diagnosis and modify treatment.
INTRODUCTION
Initial blood cultures (BCs) are recommended for patients with severe community-acquired pneumonia (CAP), especially in intensive care unit (ICU) admission, with cavitary infiltrate, leukopenia, active alcohol abuse, chronic severe liver disease, asplenia, positive pneumococcal urine antigen test, and pleural effusion [2]. The limited usefulness of initial BCs in patients with Pneumonia Severity Index (PSI) grade I-III has been reported in a previous study [3]. However, the specific contributing factors that affect the decision to change antimicrobial agents based on positive blood cultures have not been evaluated previously. In our hospital, one of the primary community hospitals in the Tokyo metropolitan area, 2 sets of BCs from almost all patients with CAP requiring admission are routinely obtained in the emergency department (ED) or outpatient department. The aims of this study were to investigate the frequency of antimicrobial agent changes based on the BC results after admission and to validate the necessity of BCs in severe CAP. Furthermore, we explored the clinical features of patients whose antimicrobial agents had been changed.
MATERIALS AND METHODS
Sample Selection
We retrospectively investigated patients admitted with CAP between January 1, 2008, and December 31, 2010. CAP was defined as the presence of symptoms of lower respiratory tract infection such as cough, sputum production, and dyspnea, along with infiltrate on the chest radiography or chest computed tomography images on admission.
To be included in this study, patients had to be 18 years or older and from whom 2 sets of BCs (2 cultures bottles [one aerobic and one anaerobic] drawn at two different times) had been obtained before starting antimicrobial agents on admission. We included patients from nursing facilities. By contrast, we excluded patients on immunosuppressant therapy (steroid therapy, chemotherapy for malignant diseases, disease-modifying anti-rheumatic drug therapy, anti-cytokine therapy), and with human immunodeficiency virus infection (HIV) as defined by the Centers for Disease Control and Prevention [4]. We also excluded patients with history of admission or antimicrobial agent use in the past 30 days.
Data Collection
Each patient’s medical record was obtained through electronic data collection. Most of the clinical variables were derived from the PSI of Fine et al. [5]. Additionally, we gathered information about the patients’ comorbidities, which were defined on the basis of documented histories from their admission summaries. We only considered the results of the initial 2 sets of BCs obtained on admission, and not the results of BCs obtained after admission.
Definitive diagnosis of illnesses after admission was made based on the results of cultures and clinical evaluation by treating doctors. The presence of bacterial endocarditis was determined based on the DUKE criteria [6]. In patient characteristics, altered mental status is not a part of the definition of “cerebrovascular disease.” Specimens were considered contaminated if only bacteria from normal skin flora were detected and treating doctors evaluated the result as contamination.
A change in antimicrobial agent management was defined as any change in the antimicrobial agent itself, or the addition or termination of agents. The rationales for change were obtained from the documentation on the patient charts recorded by the treating doctors.
The choice of initial antimicrobial agents for CAP was mainly based on the Japanese Respiratory Society Guidelines for the Management of Community-Acquired Pneumonia in Adults (the second edition, 2005). In the guidelines, empiric use of penicillin derivatives with the beta-lactamase inhibitors, Piperacillin, and cephalosporins is recommended for inpatient settings without respiratory illnesses. In case of patients with respiratory diseases such as chronic obstructive pulmonary disease, use of carbapenem or fluoroquinolones is warranted. Furthermore, in suspicion of atypical pneumonia, adding tetracyclines, macrolides, or fluoroquinolones is also recommended.
Statistical Analysis
Statistical calculations were performed using InStat Statistical Software Package Version 3.01 (GraphPad Software Inc., CA). Variables are presented as mean ± standard deviation unless otherwise stated. We used χ2 analysis and the t-test for comparison between 2 groups. P < 0.05 was considered statistically significant.
RESULTS
Patients’ Characteristics
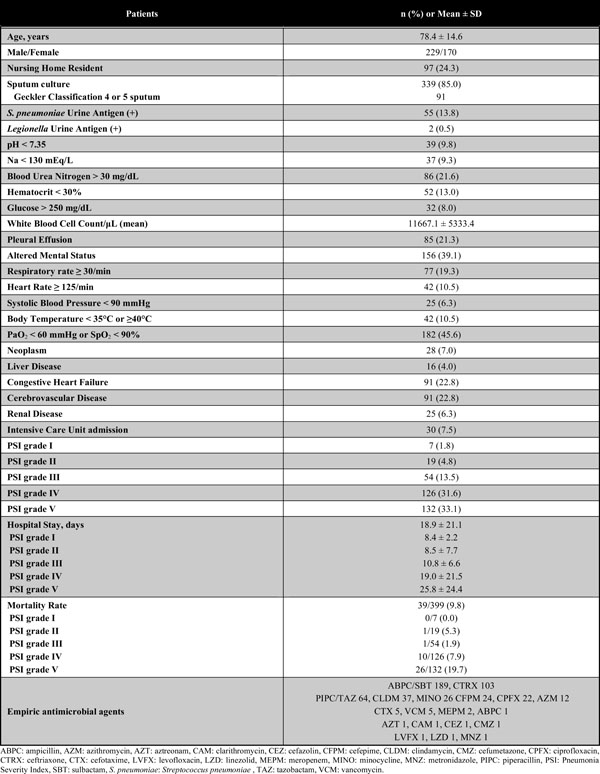
Of the 793 patients admitted with initial diagnosis of CAP, 394 were excluded (immunosuppressant use, 51; HIV infection, 4; admission 30 days prior, 141; antimicrobial agents use 30 days prior, 192; and BCs not performed, 6). The details are illustrated in Fig. (1). The remaining 399 patients (232 men and 167 women) had a mean age of 78.4 ± 14.6 years. In total, 97 patients (24%) had been admitted from nursing homes. Clinical variables as well as comorbid illnesses have also been summarized (Table 1). The Streptococcus pneumoniae Urine Antigen Test (BinaxNOW S. pneumoniae; Alere, MA) was positive in 55 out of 344 patients, while the Legionella Urine Antigen Test (BinaxNOW Legionella; Alere, MA) was positive in 2 out of 316 patients. The most common vital sign abnormality at admission was respiratory failure (PaO2 < 60 mmHg or SpO2 < 90%), followed by altered mental status. High blood urea nitrogen (BUN) level was the most common laboratory abnormality. Furthermore, the most frequent comorbid diseases were cerebrovascular disease (23%) and congestive heart failure (23%). The number of PSI grade V patients was the highest, followed by patients with PSI grade IV, and 30 (7.5%) required intensive care. The most used empiric antimicrobial agent was Ampicillin/sulbactam, followed by Ceftriaxone and Piperacillin/tazobactam.
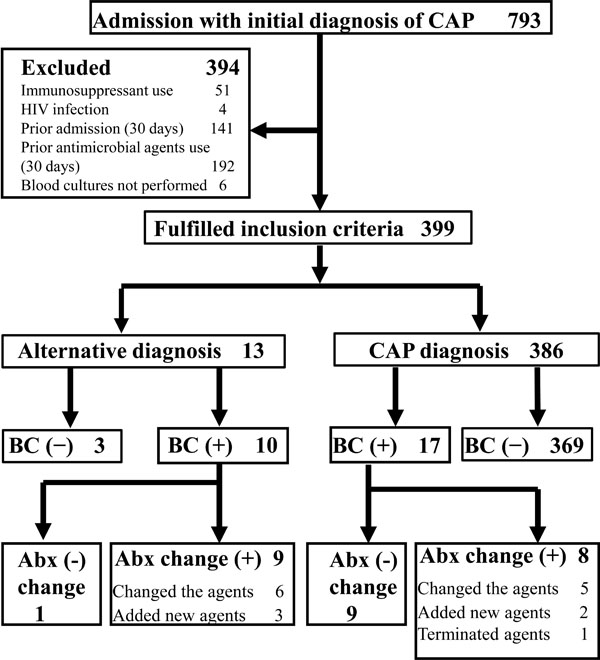
Enrollment and outcomes. Abx: antibiotics; BC: blood culture; CAP: community-acquired pneumonia; HIV: human immunodeficiency virus.
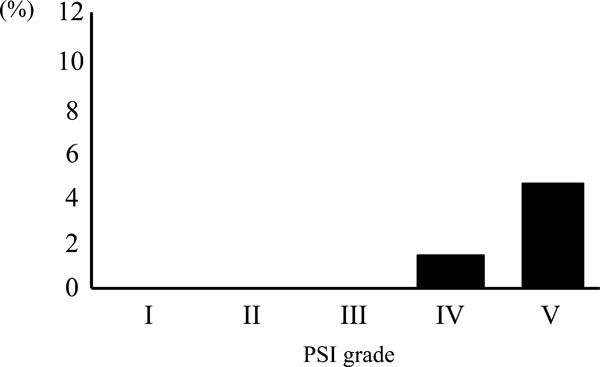
Frequency of change in the antimicrobial agents (%) based on the blood culture results with respect to the severity of pneumonia. Eleven patients changed the antimicrobial agent itself, 5 added new agents, and 1 terminated therapy. PSI: Pneumonia Severity Index.
Patient Characteristics and Underlying Conditions
 |
Bacteria Detected from the Sputum Cultures
 |
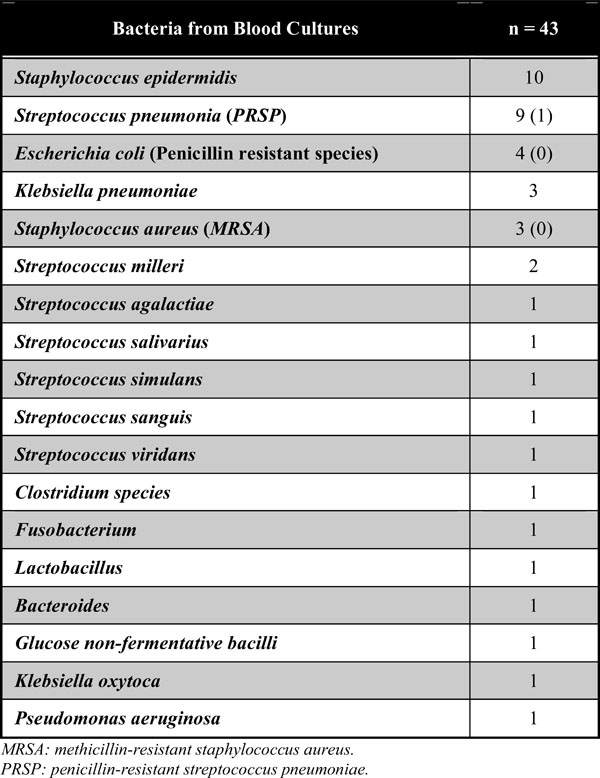
Bacteria Detected from the Blood Cultures
 |
The Specific Diagnoses, Bacteria and Drugs in Patients who Changed Antimicrobial Therapy
 |
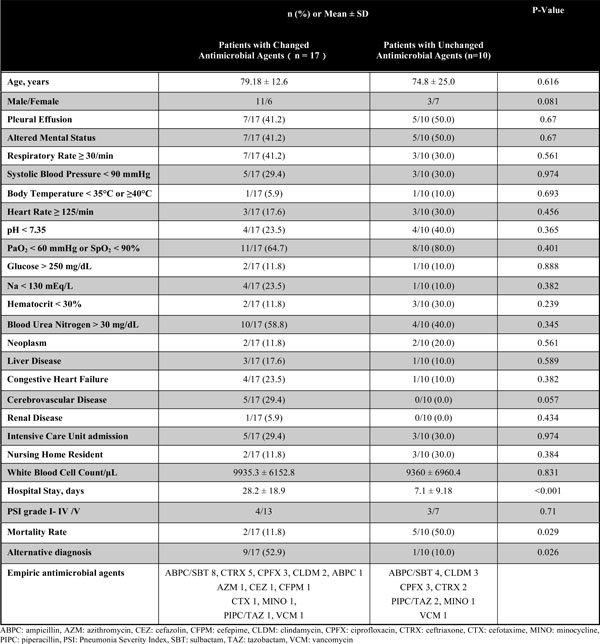
Comparison Between Patients who Changed Antimicrobial Agents and Patients who Did Not Based on the Positive Blood Culture Results
 |
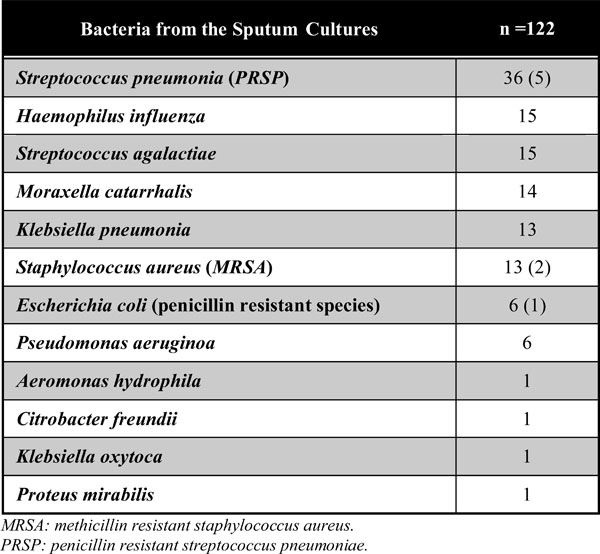
The bacteria detected from the sputum cultures (Table 2) show that most common pathogen was Streptococcus pneumoniae, followed by Haemophilus influenza and Streptococcus agalactiae.
Among patients who fulfilled the inclusion criteria (n=399), 386 were made definitive diagnosis of CAP after admission (the remaining 13 were made alternative diagnosis [non-pneumonia illnesses] based on the results of cultures and the evaluation by treating doctors after admission).
The Rate of Bacteremia and Frequency of Antimicrobial Agent Change
The bacteria detected from the BCs (Table 3) show that most common pathogen was Staphylococcus epidermidis, which is commonly considered the causative bacteria of contamination. Streptococcus pneumoniae was second most common bacterium detected from the BCs, followed by Escherichia coli. Fig. (1) demonstrates that the number of pneumonia causing positive BCs was 17 (4.4 %) out of 386 patients, whereas other etiologies (alternative diagnosis) yielded positive BCs in 10 patients (bacteremia from unknown origin: 6, urinary tract infection: 3, infectious endocarditis: 1). 12 patients were evaluated as contamination by treating doctors even though the results were positive.
Among the 17 patients with positive BCs in CAP diagnosis, 8 (Pneumonia Severity Index [PSI] grade IV; 2, PSI grade V; 6) changed antimicrobial agents based on the positive BC results (Figs. 1, 2). Therefore, 2.1% out of 386 patients with definitive CAP diagnosis (0%, 0%, 0%, 1.6%, and 4.8% out of PSI grade I patients (7), grade II patients (19), grade III patients (53), grade IV patients (122), and grade V patients (124), respectively) changed antimicrobial agents based on the positive blood culture results (Fig. 2).
Specifically, 5 patients changed the antimicrobial agent itself, 2 added new agents, and 1 terminated therapy based on the BC results (Fig. 1).
The specific diagnoses, bacteria and antibiotics in the patients who changed therapy based on positive blood culture results are shown in Table 4 (the rationale [comments] for changing antimicrobial agents was based on admission summaries for each patient). By contrast, no one changed therapy based on negative BC results.
We compared the clinical variables of the patients who changed antimicrobial agents based on the positive BC results (n = 17) with the patients who did not (n = 10) (Table 5). The former group had significantly higher frequency of alternative diagnosis after admission. Also the former group had better mortality than the latter group. However, we could not show a significant difference of severity (PSI score) between two groups. The specific empiric antimicrobial agents in both groups are also demonstrated in Table 5.
DISCUSSION
In previous studies, initial BCs for pneumonia were positive for pathogens in 7-16% of hospitalized patients [3,7,8]. As the sensitivity of sputum cultures and gram-stained sputum examinations is limited, obtaining BCs especially for pneumococcal pneumonia is warranted currently [9]. By contrast, the arguments against obtaining BCs are that the positivity is relatively low, and the rate of false-positive cultures is high. Contaminations might prolong hospital stays due to the use of vancomycin [10].
We have demonstrated that the frequency of changing antimicrobial therapy increased as the severity of pneumonia (PSI grade) increased (Fig. 2). In particular, very severe cases (PSI grade V) needed to change therapy much more frequently based on the BC results than patients with other PSI grades. Contrary to the previous study in which the frequency of antimicrobial agents change was quite high both in PSI grade IV and V groups, the effect of obtaining BCs, with the exception of PSI grade V patients, was in our study relatively negligible [2].
As shown in Fig. (1), we documented quite a few cases involving non-pneumonia illnesses (alternative diagnosis) that yielded bacteremia. This result implies that initial diagnosis of pneumonia in the ED or outpatient department tends to be inaccurate. This may result from the fact that elderly patients possibly cannot report clinical symptom to treating doctors appropriately as well as they often have more than one-infection. A previous study has claimed that false-positive BC results accounted for 50% of all positive BC results [11].
In the comparison between patients who changed antibiotics and patients who did not based on the positive blood cultures (Table 5), a significant number in the former group were made alternative diagnosis after admission (P = 0.026). This fact possibly implies that initial BCs would be helpful to find alternative diagnosis and modify its treatment.
The limitation is that this study is retrospective, which makes it difficult to obtain clear rationale for antimicrobial choices and changing them by treating doctors. Further, it is difficult to address whether changes of antimicrobial agents would have been needed. However, in a point of view for preventing multi-drug-resistant pathogens, changing antibiotics would be preferable. Further multicenter prospective study with standardized criteria upon choice of initial antimicrobial agents and changing them based on positive BC results is necessary.
CONCLUSIONS
Among CAP patients from whom BCs were obtained, antimicrobial agents were changed in 2.1% based on the BC results. In particular, the use of BCs should be limited to patients with very severe cases (PSI grade V) in hospital settings. Further, many patients are not adequately diagnosed at the ER. Therefore, BC should be drawn as the probability of changing antibiotics is higher in other diseases like urosepsis or infectious endocarditis.
ABBREVIATIONS
| CAP | = Community-acquired pneumonia |
| BCs | = Blood cultures |
| PSI | = Pneumonia Severity Index |
| ED | = Emergency department |
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
We thank Osamu Takahashi (Center for Clinical Epidemiology, St. Luke’s International Hospital) for the statistical analysis.

